Yes, here’s where I get all Jane the Actuary on you, after having dug into the statistics of STD prevalence in the US.
And as an initial caveat, of course, no one should be having sex outside of a marital commitment and nothing I write here should be understood as other than an attempt to understand what’s going on in the wider world — and, in fact, the consequences of a moral system in which sex is just a physical act of no moral relevance.
After reading about STD prevalence and thinking about the broader social context, it seems to me to be a very tough sell to (chemical contraception-using) women to say, “yes, you feel very protected from your greatest worry with respect to sex – pregnancy – by using contraception, but you must take yet another action still, each time you have sex, to avoid STDs” — especially if that action is as unpleasant or, minimally, annoying as condom usage (both due to personal dislike and the need to persuade the partner), and STDs are simply not perceived — and perhaps rightly so — as a particularly big deal, since they can be dealt with by means of regular testing and antibiotics.
(For men at risk of their partner getting pregnant, it seems to me the sell is easier: “use condoms to avoid STDs and just in case your partner isn’t taking her pills correctly, or possibly is even deceitful about it.”)
But it seems to me that what we have here is, at least in part, a matter of risk compensation.
What’s “risk compensation”? The concept that people accept a certain degree of risk in their lives, and, when one thing becomes less risky, they take more risk elsewhere. Cyclists who wear helmets bike in riskier ways, for instance.
Now, again, there’s a lot I don’t know.
Is the drop in gonorrhea over the period from 1984 to 1994 a result of the hyping of the (in the end, not really significant) risk of transmission of HIV to women through heterosexual sex? (Is there some weird epidemiological reason why chlamydia infections didn’t merely increase but skyrocketed during this time frame?) Are some women responding with a sense of “they tricked us” when that turned out not to be the case?
What are the real risks of these two diseases? (Note that the politically correct terminology is “infection,” all the better to reduce stigma or, really, worry or concern.) In my online searches, which are admittedly not as extensive as if I were a scholar examining the research, I am not seeing anything along the lines of “if you have multiple partners/if you’re over/under 25, etc., your risk is X%.” And I’m not seeing anything that reports on relative differences in risk for, say, sex workers or drug users or the like. I’m also not seeing anything on whether there’s any difference in the relative likelihood of transmission for either of these two diseases, or whether different types of activities elevate the risk for one or the other.
Incidentally, the reason why all women under age 25 are recommended for testing is at least in part that they are at greater risk due to their physiology; for whatever reason their bodies are more susceptible to these diseases, not simply that they are more likely to engage in sex irresponsibly and can’t be trusted to answer a screening questionnaire honestly.
But, again, going back to the fact that LARCs are now being so heavily promoted, is a woman who wishes to have multiple-partner sex necessarily making a poor decision if she decides it’s no big deal to need antibiotics every now and again, and to be sure to be tested regularly? We know that pro-abortion folk say things like “it’s perfectly normal to have an abortion every now and again as a part of having an active sex life.” Is it a reasonable expectation on the part of public health folks to expect that sexually-active folk should comply with the instructions being given on how to avoid STDs that are curable, especially when there are no concrete statistics being shared about what their risk actually is (compared to contraceptive chemicals and devices about which failure rates are heavily promoted, as is the likelihood of pregnancy without any such use)? And, of course, some of the risks are more hypothetical consequences that could affect others: “chlamydia can cause PID which can cause infertility if not treated early enough, so you should use condoms so as to avoid passing it on to someone who might pass it on to someone for whom it might matter, even if you personally don’t want to have kids” or “gonorrhea might in the future become resistant to antibiotics, so you should use condoms to prevent that from happening and future generations suffering.”
Many years ago, in fact, I engaged in a debate about these risks, and the response I was given was, “life has risks and we all accept that; to say ‘no premarital sex because you might get pregnant or get an STD’ is the same as saying, ‘don’t drive because you could have an accident.'” And, of course, it points to the weakness of trying to argue against nonmarital sex purely because of the risks of undesirable outcomes (especially if you’re arguing against someone who’s A-OK with abortion).
So, again, not an expert, but it seems to me that those experts can yammer all they want about the need for more money for public health programs all they want but if they don’t take into account human behavior, it’s hard to make progress.
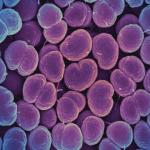
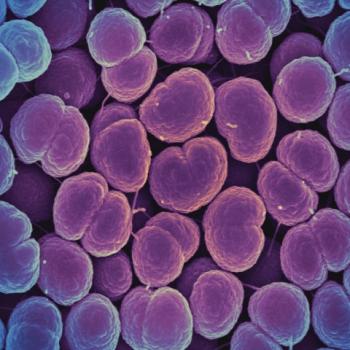
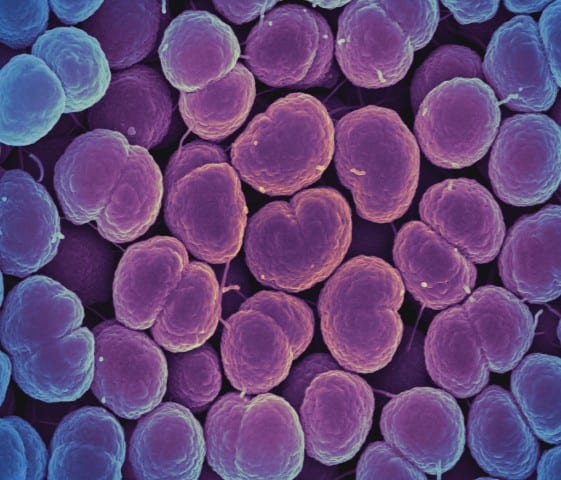
Image: Colorized scanning electron micrograph of Neisseria gonorrhoeae bacteria, which causes gonorrhea. Credit: NIAID; https://commons.wikimedia.org/wiki/File:Neisseria_gonorrhoeae_Bacteria_(16221300454).jpg