In the post “Circle Round”, I asked other practitioners with disabilities to join me in learning about different types of socioeconomic systems and how they have been implemented in other nations. Currently in many nations around the world, people are gathering in occupations and protests over these issues. I would like these series of posts to be our opportunity to think about important aspects of society which include: trade, knowledge, interpersonal relationships, culture, health, safety, and natural resources (air, water, food). These are very broad topics so we’ll take each one a step at a time.
Healthcare is an important issue for people with chronic and even temporary disabilities or illness. There are sixteen nations that participate in the Organization for Economic Cooperation and Development (OECD) and have some form of multi-payer or national healthcare. OECD provides a lot of research and statistics so that’s why I’m focusing on those nations. By reviewing how other nations handle their healthcare, I want to end the myths that multi-payer or national healthcare:
1. is inadequate with long waits and substandard aide
2. is a tax burden on citizens
3. bankrupts nations
The Physicians for a National Health Program offer health statistics from many of the OECD nations and clear explanations why national healthcare would succeed in the U.S.
The interviews are about more than just healthcare though. We’ll find out what type of government some of these nations have and how people of different religions treat each other. If you live outside of the US and would like to participate, let me know. I’ll send you some ideas about what to include. Email me at tara.miller21 (at) gmail.com or leave a message in the comments.
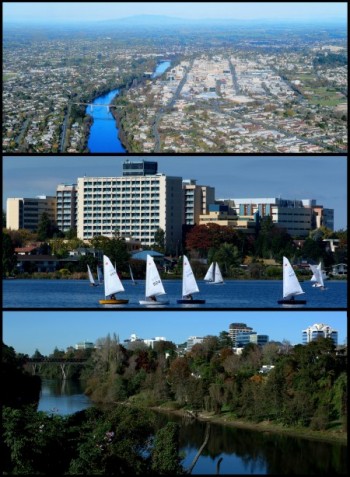
IMAGE: Montage of Hamilton City. Features Hamilton from the air, Lake Rotoroa and the Waikato River. All images courtesy of the Hamilton City Council. Wikimedia Commons
New Zealand
On a national level, New Zeland is a parliamentary democracy and constitutional monarchy under the Sovereignty of Queen Elizabeth the II. Parliament has only one chamber which is the House of Representatives. Specialized departments of the government are run by ministers. Ministers are elected members of Parliament who are appointed to a ministry. Then there are regional, city, and local councils. New Zealand was the first country with a free market economy to achieve universal coverage. This occurred in 1941. New Zealand spends 8.1% of its GDP on health care. (Wikipedia)
Lusi, in New Zealand, offered to discuss her nation’s healthcare system. I was really impressed by the amount of research she put into our e-mail interview.
Masery: Where do you live in Aotearoa/New Zealand?
Lusi: I live in the city of Hamilton/Kirikiriroa (pop. 180,000), in the north/central area of the North Island. It’s the main centre of our region and isn’t known for much of anything, but we have a university, a tradition of dairy farming, and a reputation for generalised apathy (hence the gently ironic nickname, “Hamiltron: City of the Future”).
Masery: What is the land (geography) like?
Lusi: Our region, the Waikato is surrounded by volcanic and geo-thermal areas. It has a lot of swampland, several small volcanic mountains (extinct/dormant), and the Waikato River flowing through it, north-west to south-east. Hamilton is on the banks of the Waikato, and much of the land is reclaimed swamp (bad news for asthmatics!). Burning of native forest in the late 19th/early 20th centuries has provided a lot of pasture for sheep and dairy farming. Flora is a mix of NZ natives (trees/grasses) and introduced European species.
Masery: Were you born in Aotearoa/New Zealand?
Lusi: Yes, I was born here in Hamilton, and after moving to a different city, aged 8, I returned here after I left high school.
Masery: How long have you been a Pagan?
Lusi: I have had an instinct toward animism my whole life, but I gradually came to identify as pagan from the age of thirteen.
Masery: Do you practice a specific tradition of Paganism?
Lusi: I am Heathen, but from online conversations, I’ve come to believe that that word has slightly different connotations in the US! I am not Asatru, but I do worship the Gods of the pre-Christian Scandinavian/Germanic peoples.
Masery: What drew you to that path?
Lusi: I was beginning to explore Celtic Neo-Paganism (via study, rather than practice), and that indirectly led me to friends who were Heathen. Whilst I didn’t join their group, their conversations led me to explore Heathenry on my own, and as I did, the Gods simply made Their presence known to me, to the point that declaring myself Heathen became nothing more than a fait accompli.
Masery: In America, sometimes people don’t know their neighbors. What is your neighborhood like?
Lusi: I live in a “heritage suburb” on the riverbank, on the opposite bank to the city’s Central Business District, and bisected by two main thoroughfares. From what is largely a mix of Victorian/early 20th century buildings and cheap mid/late-20th century developments, it’s an eclectic mix of historic village charm and downtown seediness. We’re beginning to get new property developments, but they’re resisted by some, on the basis of “village character” and/or traffic congestion. We also have some beautiful park areas, especially along the river bank, and the main street and community park are known for their huge, old oak and plane trees.
We have a reasonably large immigrant population (African, Polynesian, Asian, Middle-Eastern) mixed in with native Maori and those of European descent. There is a wide variety of socio-economic groups in the neighbourhood, from wealthy professionals to the almost-indigent. The population also shifts due to the high turn-over in student numbers from the near-by university, and from immigrants using temporary cheap rentals prior to settling more permanently elsewhere. The economic divides, the common language barriers, and the natural laid-back reticence of New Zealanders mean that people are generally friendly and polite, but strangers don’t tend to be overly demonstrative to one another. I suppose I would say I’m on nodding terms with some of my neighbours, and on casual-chat terms with a few more.
Masery: Do you have children? If so do they attend a public or private school?
Lusi: I have one child, who attends a State-Integrated Catholic school. (State-Integrated means that the government pays teaching salaries and some teaching costs as they would for a public school, but the expenses of land, buildings, and “special character” teachings must be met by the site owners – in this case, the Church – via private fees.)
It might seem strange, for a pagan to send their child to a Catholic school, but my family has attended there for many generations, and the quality of not only the tuition, but also their community and student support, is excellent. I’m told, also, that NZ Catholic schools are nowhere near as strict or dictatorial as those in other parts of the world. NZ’s public schools are residentially-zoned by the government, so the choice of other schools to which I could have applied was limited anyway.
Masery: If a student attends a public school in the US, they can only enroll in
the school district where they live. New Zealand seems to be similar in
that way.
Lusi: NZ schools often have an “unzoned quota”, where people from out-of-zone can apply for one of a limited number of places – sometimes it’s a lottery system, sometimes it’s application/interview-for-suitability. I have no idea if that’s found in the US.
Masery: Have you experienced discrimination because of your religious beliefs?
Lusi: Not directly – NZ is quite secular, so religion doesn’t really have an overt effect in such things as public education, health care, or social welfare. I’m not terribly demonstrative about my faith – I don’t deliberately lie about it, but I see no reason to unnecessarily bring it up (NZ is one of those places where one doesn’t generally discuss politics, money, or religion in depth, except with friends/family – and even then it can be touchy!).
However, I (and others I know, of various faiths) have experienced a lack of accommodation – cases where a secular humanist or Christianized assumption has left us having to specifically request different treatment, or opt out of social events, etc. Most of the time the difficulty seems to rest on cultural ignorance, rather than malice.
Actually, come to think of it, most of my interpersonal difficulties have come from the fact that, for me, religious beliefs naturally manifest as daily choices. For many of the Abrahamic/Agnostic/Atheist people around me, divorcing their faith/philosophical/cultural beliefs from some, or all, of their every-day actions is easy, if not obvious. For the devout (of *any* faith or culture) the very act of requesting special accommodations or exceptions can cause annoyance of the “why are you making things difficult?” variety.
A very practical demonstration of this was a fight I had with one authority figure – over disposable cups at a fundraiser. :p She wanted me to bring them as my contribution; I couldn’t bring myself to deliberately buy a one-use, non-biodegradable plastic product (I offered alternative help, but she was having none of it!). To me, it was a natural extension of my beliefs. To her, I was being annoying and overly precious about something that didn’t really matter. The depth of my belief was irrelevant to her way of thinking, except in that it caused her inconvenience.
I suppose it’s the lack of moral relativism that causes the upsets, rather than the fact that I belong to such-and-such a faith. I say I am Heathen; they respond briefly with polite disbelief or humourous contempt. I act like a Heathen; they get irritated and argumentative. C’est la vie.
Masery: If someone were to become unemployed, how would they seek help?
Lusi: They would apply to Work & Income NZ (WINZ), which is a division of the Ministry of Social Development. Their individual circumstances would dictate for what assistance (if any) they were eligible, and consequently their stand-down period. Emergency assistance is often available where need can be demonstrated; this may include food vouchers, transport assistance, and/or financial loans (paid back at 0% interest) or non-recoverable grants (not paid back).
If the unemployment were due to accident or injury, the person could file a case with the Accident Compensation Corporation (ACC), a Crown agent that pays for or subsidises lost wages, medical expenses, rehabilitation, retraining, etc. ACC is funded by taxpayers and employer levies.
Masery: Are there private or religious charities?
Lusi: There are a great many private and religious charities and not-for-profit organisations in Aotearoa/New Zealand. Most of the nation’s foodbanks, charity shops, and many shelters, are run by church groups, whereas many of the advocacy/community support groups are private not-for-profit societies. International groups like the St Vincent de Paul, Red Cross, Rotary Club, and the Salvation Army have higher profiles, but every city has smaller independent charities addressing local needs. It is also very common for charities to be run by Trusts, and to receive partial funding from the Government and/or corporate sponsorship.
Masery: The New Zealand health care system is made up of many different organizations and committees. I don’t understand them all. Could you offer a brief explanation of how the Regional, Crown, primary health organizations, and local non-profits work together to provide health services? http://www.health.govt.nz/new-zealand-health-system/key-health-sector-organisations-and-people
Lusi: All public health care is run under the auspices of the Ministry of Health, but health care has been increasingly corporatised since the 1980s. Successive Governments have attempted to split the governance of the health care system away from its management structure, with mixed results.
Crown Entities are part of the State Sector; that is, they may be Crown agents (acting on behalf of the Govt), autonomous Crown entities (headed by the Govt but self-managed), or independent Crown entities (run separately and treating the Govt as a third party). The three divisions exist for transparency and accountability (e.g. those that monitor the Govt’s performance and accountability are independent entities, those designed to provide unbiased advice are autonomous). Many Crown entities are concerned with policy/advisory issues (e.g. the Health & Disability Commissioner), whilst others provide direct services to the public on behalf of the State (e.g. the Accident Compensation Corporation).
One Crown agent of note is Pharmac, which manages the Government’s pharmaceutical budget on behalf of DHBs and decides which medicines are funded by the government. Medications supplied via Pharmac are often subsidised, many to provide a flat rate of $3 per item to the customer.
The “top tier” of health care is the non-profit District Health Board. There are currently 20 DHBs, each covering a geographical region of the country. Public funding is provided by the Ministry of Health, and is apportioned based on the size of the district’s population, and their mix of ages, ethnicities, socio-economic statuses, etc. Each DHB is assigned achievement objectives by the Ministry, but has discretion in how they are achieved. DHBs run hospitals and specific-care providers such as mental health facilities, birthing centres, and community health care programmes (school health checks, social workers, out-patient clinics, etc.).
Next we have Primary Health Organisations, which are local groups to which non-hospital medical providers often belong – the most common are, of course, GPs/family doctors, and nurses. Enrolling in a PHO is voluntary, and non-enrollment doesn’t affect the services a patient may receive. PHOs are funded by their local District Health Board, and that funding subsidises the cost of services; this results in a lower, often standardised, fee for patients. The majority of care for children is either free or low-cost.
Emergency hospital care is provided by the District Health Boards. In-hospital accident and emergency care is free. Ambulances are subsidised, with patient costs varying by area – two DHBs maintain their own ambulance services, with St John and the Wellington Free Ambulance covering the rest of the country. Despite subsidies from the government, both land and air ambulances rely heavily on volunteer services, sponsorship, and fund-raising.
Private health insurance and private hospitals have emerged gradually over the past 20 years, but the majority of New Zealanders still rely primarily on public health care.
Masery: Do you think you have adequate health care?
Lusi: At the moment, I think my main day-to-day health concerns are well addressed – my primary health care is affordable and pharmaceutical subsidies are sufficient. I am quite happy with my access to, and service from, the various Hospital Outpatient Clinics I have needed over the past five years. Secondary care (specialist) waiting lists are a little long (averaging 6-12 months for non-urgent cases), but they are apparently better than in many parts of the world. I’ve been personally lucky in averaging 3 months for the few times I’ve needed a referral, however it’s currently 4 months (and counting!) since my GP referred my child to the paediatrician, and we don’t even have an appointment date yet!
However, I have greater concerns with two areas; after-hours health care, and dentistry. After-hours non-emergency care is expensive; to see a doctor after 6pm or in the weekend can cost anything from $45 to $100. This means either delaying medical care for anything up to 72 hours over the weekend, or clogging up the Accident & Emergency rooms of public hospitals with non-emergency complaints (having Type 1 Diabetes, it can be a bit of a guessing game as to whether a problem is, or is not, an emergency “right now”, or whether it’s likely to become so before 8:30am Monday! There is often a bit of guilt involved in trying to make that call – take the risk and stay home (with only a 9-year-old for support), or err on the side of caution and potentially waste everyone’s time/resources, and delay treatment for the person behind me in the queue?).
Dentistry is free for children under 18, but non-accident/emergency dentistry is usually unsubsidised for adults (some DHBs provide subsidies for targeted low-income patients, but not all). There are a great number of people who simply do not vist the dentist once they turn 19; visits average $50-$150; other costs range from basic extractions averaging $180-$200, to crowns at around $1,000 each. As a diabetic, this is a fairly scary concept for me; diabetes pre-disposes one to oral health problems, and oral health problems (or any infections) can cause diabetic complications – a vicious circle.
Masery: Are you familiar with Rongoa (Maori Medicine)?
Lusi: Not particularly – I was aware that traditional medicine existed, but not the name! I have been tangentially aware of some traditional herbal treatments via word-of-mouth, but previously lacked any other knowledge. Looking at it now, I see that it involves not only the herbal medicine of which I was aware, but also (at least) massage, prayer, and counseling.
Masery: Are there Rongoa clinics and is it available in public clinics?
Lusi: Information on Rongoa seems patchy, as there is no national regulatory body. Many Rongoa Māori practitioners seem to be based in private (often “alternative healing”) clinics rather than public clinics.
Masery: Does the HFA (Health Funding Authority) cover Eastern medicine or Rongoa?
Lusi: According to the Ministry of Health, as of 2009 there were 16 government funding contracts for Rongoa services (I’ve found no newer information.) Eastern (and other “alternative”) medicines can be covered by government funding, but only if it is “essential treatment” provided by a registered medical professional and, in the case of ingested treatments (herbs, supplements, etc.), there is no equivalent subsidised “mainstream pharmaceutical treatment” available.
Masery: Please summarize public healthcare benefits in New Zealand, especially for the disabled.
Lusi: People who are unable to work due to illness or injury lasting more than six weeks can apply to WINZ for the Sickness Benefit. Those whose illness or injury is ongoing or permanent can apply for the Invalid’s Benefit. These are based on a “basic cost of living” similar to the Unemployment Benefit and, like the UB, may be “topped up” by additional benefits (Accommodation Supplement, etc.) depending on the client’s circumstances.
There is also a Disability Allowance for those with an ongoing disability or health problem, which pays a moderate weekly amount (over and above other benefits or subsidies) for ongoing costs such as medications/treatments, medical alarm monitoring, or assistance with home and garden maintenance. Those with a long-term physical disability may qualify for a Modification Grant, which pays for special equipment or workplace alterations that will enable them to return to or accept employment. The Disability Allowance and Modification Grant are available to those on a WINZ benefit or low income. The Government has recently announced a “Disability Innovation Fund, for “innovative projects from the employment sector, NGOs or disabled people’s organisations to get disabled people into jobs or to retain them in jobs”, which is targeted at people who are not eligible for assistance from existing employment programmes, WINZ, or ACC.
Those on low incomes/benefits are assisted by the Community Services Card (CSC), which provides subsidies on doctors’ fees and prescriptions. While GPs’ (General Practitioners) costs vary, depending on area and patient income, the CSC offers a significant benefit – someone with a CSC might pay $10-$17 for an appointment, while those without average $40-$50. Any person with a medical condition requiring regular ongoing treatment who doesn’t qualify for the CSC may qualify for a High User’s Card, which subsidises doctors’ and other medical costs. Anyone who fills more than 20 prescriptions in a year gets a Prescription Subsidy Card, which gives them free prescriptions for the rest of that year.
Many organizations – private, public, and volunteer – offer travel assistance or subsidies for those needing to attend health care providers. WINZ can cover travel costs in certain circumstances, either by grant or loan. Many individual hospitals and outpatient clinics employ free or low-cost shuttles to transport patients, especially those from rural areas and/or with mobility issues.
The government provides a special funding pool for one-off, high-cost treatments that cannot be met from within the existing NZ health service (examples are rare specialist operations, gender-reassignment surgery, some cancer treatments, organ transplants, and complex cases of otherwise-routine procedures). Referrals for this service must come from a medical specialist and meet specific criteria.
Mental Health & Addiction services are not well-subsidised at the community/self-referral level; a Disability Allowance application may be made with WINZ for help with counselling fees, but this is generally limited to 10 visits or less per application. In certain circumstances, trauma or abuse victims/survivors may be granted money for counselling by ACC. Services are comparitively better at the public health/professional-referral level (outpatient clinics and care facilities).
Disability Services is a branch of the Ministry of Health that provides assistance to people under 65 years with a long-term or permanent disability. They do not fund disability support services for people whose primary needs are driven by a personal health condition, mental health, health conditions more commonly associated with aging, or injury/accident covered by ACC. Most of their services are contracted to private companies, but are publically-funded. Disability Services provides a range of assistance, including housing/vehicle alterations, home-based support for living, Supported Independent Living programmes, and advice/support/rehabilitation services.
The government provides a means-tested subsidy for the elderly and others requiring residential care. Over 65s may get a hearing aid subsidy from the government, and if they do not qualify for a WINZ Disability Allowance, they can apply to the DHB for help with home maintenance.
Parents who are caring for a child with a disability (either at home, or in a care facility for which they must meet costs) get a non-means-tested Child Disability Allowance (currently just under $50/week) from WINZ. Respite care is available from Child, Youth, & Family Services (Ministry of Social Development) for the caregivers of children with disabilities, and is often available also for caregivers of children with behavioural challenges. A current challenge for many is the fact that those caring for family members with disabilities are not paid for doing so, while those caring for non-family members are – there is a case currently before the courts addressing this issue.
Housing New Zealand Corporation is a Crown agent that provides housing and housing services to people in need. They have a Suitable Homes Service that works with disabled people to find or alter housing that meets their particular needs. Housing Corp also operates a Community Group Housing Programme that acquires and rents houses to organisations providing support, advocacy and day activities for disabled people. In practice, need often outstrips availability, however.
There is a national scheme called Total Mobility, operated by local authorities and jointly funded by central and local government, which is aimed at better mobility for those with serious mobility constraints. It offers vouchers for 50% reductions on taxi fares. Many local governments offer public transport subsidies for the elderly and people with mobility difficulties.
Masery: How much of your pay does the national government take in taxes? Are you taxed by regional and local government, too?
Lusi: NZ income is subject to withholding tax (i.e. tax is withdrawn prior to the employee receiving pay/benefits). Income tax rates are variable, based on income and circumstances. My income tax rate depends on my ability to find part-time work; on a single parent’s benefit it’s the Main income rate of 17.5%, but when working 20 hours or more per week I pay Secondary income tax of 29.54% on wages (including automatic student loan repayments), plus an ACC levy of 2.04% of gross income (as well as having my WINZ benefit reduced and paying 17.5% on the benefit I do receive).
Local and regional government taxes (“rates”) are calculated on property values/usage. Since I don’t own property I don’t pay them directly, but contribute to the property’s rates through paying rent.
Masery: What is your opinion of local government?
Lusi: Most local governments in New Zealand seem to struggle with poor civic infrastructure and a growing pressure to increase corporate-style management systems (but they don’t receive a lot of support to achieve this).
My own local government has in the past been criticised as a “good old boys network” and has had problems with transparency and accountability (especially in areas of property development). There have also been recent problems with large amounts of money being sunk into major public events and civic venues (some of which have been actively opposed by the populace) that have not paid off as promised. It seems to be part of a new emphasis on “brand recognition” of cities and regions, which along with the current Recession, has diverted attention and funds away from “unprofitable” areas like low-income housing, assistance for the elderly and those with special needs, and community support programmes, and into commerce and sports/tourism.
There have been improvements made in some areas, such as transportation – better disabled access on buses, lower ticket prices, improved parking facilities – but grass-roots support organisations are not doing as well as they might. Other improvements are being made by the new Mayor and the Council, but I think it will be a long uphill trudge for both the Councillors and the public, with no guarantee of a positive result.
Masery: What is your opinion on New Zealand’s parliament?
Lusi: Since we just finished national elections, that’s an interesting question. Our parliament is run under MMP (the Mixed Member Proportional system), which allows smaller political parties a much greater presence in the House. Whilst MMP allows better representation, it also means that very small parties can wield a disproportionate amount of power (for example, two parties (Conservative-Right and Conservative-Centrist) currently have only one Member of Parliament each, but those two MPs hold the balance of power that allows the Government to hold the majority in Parliament, and have bargained that for concessions on health care, welfare, and education issues). Thankfully the way that MMP is run is going to be under review shortly, so that may be eventually fixed.
The previous Centre-Right coalition government retained a bare majority in the election, so I’m not terribly optimistic – they have policies which include tighter conditions on social welfare and student benefits, and increased privatisation and private-contract outsourcing of health care, education, and social welfare services. They seem far more focused on getting disabled and health-compromised people “well enough to work” than “well enough to live”.