During arguments before the Supreme Court last week, Texas Solicitor General Scott Keller stated that an amicus brief filed by Former Abortion Providers and the National Association of Catholic Nurses contested the settled fact that going through childbirth is etaore dangerous for a woman than having an abortion. Curious, I looked this amicus brief up, and what I found was illuminating. I’ll be writing a series of three posts looking at the rhetoric and statistics used in this amicus brief to argue that abortion is more dangerous than is generally understood.
The first thing I noticed was how misleading the brief is in its use of language. I had barely started reading when I came to this, for instance:
A. H.B. 2 Is Necessary Because of the Documented Physical Risks and Fatal Complications of Medical Abortions.
Both the FDA(2) and Danco, the drug manufacturer,(3) have acknowledged that RU-486 poses health risks for women. The Mifeprex drug label acknowledges that “[n]early all of the women who receive Mifeprex and misoprostol [the RU-486 regimen] will report adverse reactions, and many can be expected to report more than one such reaction.”(4)
On its face, this sounds awful! Nearly every single woman who takes the medical abortion pill has adverse reactions?! Presuming this number is correct, how did this pill get to market?! Women are being endangered! But hang on a second. Do you see that itty bitty little footnote? Check it out:
4 Id. (stating adverse reactions include abdominal pain, uterine cramping, nausea, vomiting, diarrhea, pelvic pain, fainting, headache, dizziness, and asthenia).
Yes. Yes really. The aforementioned “adverse reactions” to the abortion pill include abdominal pain and uterine cramping. Not so scary after all, huh?
Frankly, the only thing strange about the information presented here is that there are some women who take the medical abortion pill don’t have abdominal pain and uterine cramping. The medical abortion pill induces what is essentially a late period, and you know what? Most women who have periods experience abdominal pain and uterine cramping! How severe this is varies from woman to woman, but even my fairly painless periods have always come with at least some amount of light cramping!
This information is buried in a footnote. Most people don’t read footnotes. The casual reader will likely be shocked to hear that nearly every single woman who takes the medical abortion pill reports adverse reactions, because it makes that drug sound far more dangerous than it actually is. This is disingenuous, and it engages in scare tactics to the extreme. Besides, every time I watch a TV show I see advertisements for prescription drugs with a list of possible side effects that seemingly takes ages to read.
You know what? We women are responsible enough to make our own informed medical decisions, and you better believe abortion clinics go over possible side effects just like any other doctor’s office. I’m amazed by how much anti-abortion rhetoric assumes that women don’t know what’s best for them or that they aren’t educated or intelligent enough to make their own informed decisions.
Next, here is probably the most egregious example of the amicus brief making grandiose claims that are little more than assertions:
I. MEDICAL ABORTIONS HAVE DANGEROUS AND FATAL PHYSICAL COMPLICATIONS, AND THEREFORE, TEXAS IS JUSTIFIED IN PROVIDING SAFETY MEASURES TO PROTECT WOMEN.
Medical abortions such as the RU-486 regimen pose a substantial risk to the physical health of women including severe complications and the risk of death. The scientific studies demonstrate a substatially higher risk of death from infection than surgical abortions or childbirth. There is also a high failure rate of the drug requiring additional surgeries and medical care. Therefore, the protections of H.B. 2 are necessary to protect women.
Given that this is the introductory section, there is no footnote provided, and we’ll look at some of the brief’s footnoted studies in part two of this series. I want to take a moment, though, to point out how just how out of touch with actual scientific data these claims are, because we do have ways of comparing mortality rates, and they don’t say anything like what this brief says they do. See here, for example.
Take a look at the numbers in this utterly fascinating chart:
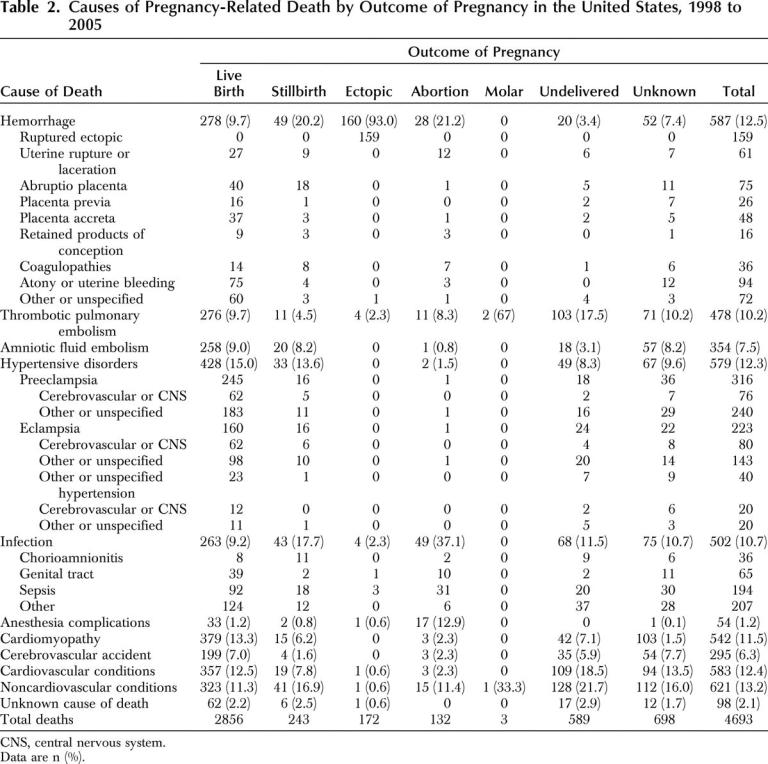
This study relied on an analysis of death certificates for women who died during or within one year of pregnancy from 1998 to 2005. According to this study, 3% of the pregnancy-related deaths identified and analyzed using this data were associated with abortion, whether spontaneous or induced, as the pregnancy outcome. In other words, this 3% includes miscarriages. The remainder of the pregnancy-related deaths identified and analyzed during this period were associated with other outcomes, including live births and stillbirths.
Note the total number of maternal deaths associated with abortion as the pregnancy outcome—132. This number sounds high until you remember (a) that it is the combined total for eight years; (b) that an average of 570 pregnancy-related deaths not associated with abortion occurred each year during the years covered by the study as compared to an average of 16 pregnancy-related deaths associated with abortion each year; and (c) that approximately 1.2 million abortions occurred each year as compared with 4 million live births.
Approximately 1.2 million abortions were performed each year from 1998 to 2005, adding up to a total of roughly 9.6 million abortions. Even if we assumed that all 132 deaths were related to induced abortions, as opposed to spontaneous miscarriages, the overall mortality rate would still be only 1.4 per 100,000 abortions, as compared to the overall 12.0 to 16.8 pregnancy-related deaths per 100,000 live births reported by the study for those years. In other words, the risk of death when carrying a pregnancy to term is ten times greater than the risk of death associated with having an abortion.
Even this comparison likely exaggerates the abortion-related fatalities, actually, and many other studies put the risk of death due to abortion even lower—remember that the numbers in the chart above include deaths related to spontaneous abortions, or miscarriages, and not just deaths due to induced abortions. Further, remember that these numbers would include deaths related to all induced abortions, and not just first trimester induced abortions (which are the most safe). Finally, it may be worth mentioning that the mortality rate associated with carrying a pregnancy to term has risen since this study was conducted.
But let’s return to the particular language used in the amicus brief. Is the risk of infection, specifically, (a) higher for medical abortion than for surgical abortion and (b) higher than for childbirth? This is harder to tell using the numbers in the chart above because they don’t differentiate between medical abortions and surgical abortions. But I do want to note that death due to infection makes up only 10% of the deaths associated with childbirth in the chart above while every death due to a medical abortion that I’ve read about was due to infection. In other words, comparing the two based only on the rate of death due to infection is more than a little bit deceptive.
Oh, and a quick note on the high failure rate of medical abortions—in my experience, clinics are up front with women about the failure rate, and women choose medical abortions knowing they may need to come back into the clinic (generally at no cost to them) if the abortion does not complete. At the Planned Parenthood where I volunteered, women who had medical abortions were always scheduled for followup visits, which could take place at Planned Parenthood clinics closer to their homes, to confirm that that the abortion had completed. In addition, they were always sent home with a packet of papers to take with them to the hospital in case of emergency, so that medical personnel there would know what medication they had taken.
But let’s look at one more bit from the amicus brief.
In 2011, the FDA issued a report on the post- marketing events of RU-486.(16) The FDA reported that there were 2,207 adverse events (complications) in the United States related to the use of RU-486, including hemorrhaging, blood loss requiring transfusions, serious infections, and death.(17) Among the 2,207 adverse events were 14 deaths, 612 hospitalizations, 339 blood transfusions, and 256 infections (including 48 “severe infections”).(18)
When I first saw this paragraph, my response was yikes, 14 deaths in 2011?! That’s a bit more dangerous than even I thought it was! But then I checked the footnote.
16 Food and Drug Administration, Mifepristone U.S. Post- marketing Adverse Events Summary Through 04/30/2011 (July 2011), available at http://www.fda.gov/downloads/Drugs/Drug Safety/PostmarketDrugSafetyInformationforPatientsandProviders/ UCM263353.pdf (last visited Jan. 14, 2016).
17 Id.
18 Id.
That word “through” suggested to me that all was not as it seemed, and I looked up the document referenced in the note. It turns out that there had been 14 deaths since 2000. That sounds a little bit different, now, doesn’t it?
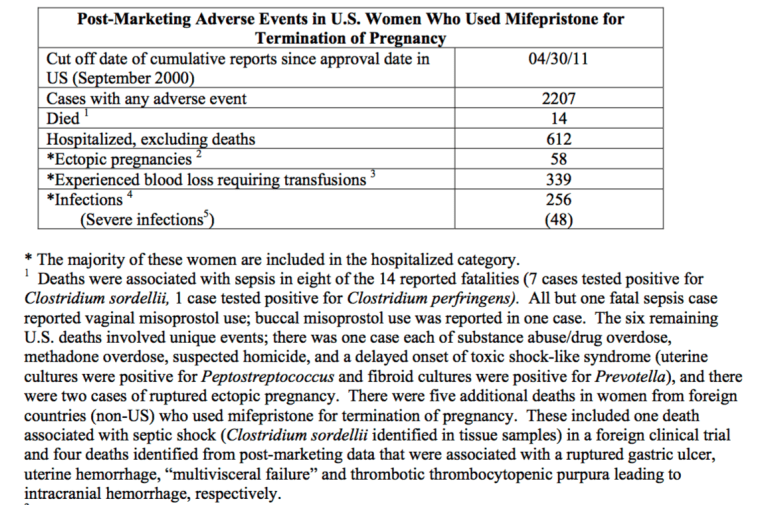
According to the document, an estimated 1.52 million women had taken mifepristone as of April 2011. I’m no expert, but 14 deaths and 612 complications resulting in pregnancies out of 1,520,000 medical abortions over the course of 11 years sounds like a fairly low rate of problems. But of course, that’s not how the amicus brief puts it—and that’s rather the problem. By omission, they’re engaging in what looks like fairly deliberate deception. The problem is that the language is just technical enough—and just footnoted enough—to make it sound like it must be true.
In the next two posts, we’ll look in more depth at some of the footnotes backing up—or not backing up—the brief’s claim. But in many ways the problem here is the one we see with creationism—opponents of abortion have learned to use technically language and a heavy dose of footnotes (sometimes to mere webpages, other times to studies that don’t say what they say they say) to mislead their reader. Think about what they’re doing here—they’re trying to convince the justices on the Supreme Court (and anyone else reading their brief) that medical abortions, with their extremely low complication rate, are more dangerous than childbirth, which typically takes place in a hospital because of the very real risk that something might go wrong.
Ask yourself this—have you ever known someone who had to have an emergency c-section? The odds are, your answer is yes. Now remember that only 612 out of 1,520,000 medical abortions required hospitalization. That’s 1 in 243. Believe me, I am all in favor of protecting women’s health and improving their access to effective care. But arbitrarily deciding that you get to decide which methods are safe and acceptive for women to access based not on sound numbers and best practices but on deceptive use of statistics does neither.