While spending time on google, I came upon this headline from an anti-abortion website last year: Court Records Indicate Nearly 1,000 Abortion Patients Likely Hospitalized Annually in Texas. The article explained that during the year 2011, a full 940 women were hospitalized in Texas due to complications from abortions. These numbers came out during court proceedings over new abortion restrictions. Of course, the article made this number out to be apocalyptic.
“Information in this decision has forced us to crunch the numbers,” said Troy Newman, President of Operation Rescue. “Our calculations based on conservative estimates indicates that nearly 1,000 women might very well be hospitalized each year in Texas alone. That number is completely unacceptable.”
The article included this image offering a breakdown of these hospitalizations:
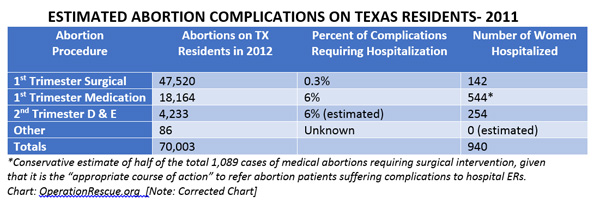
A total of 940 hospitalizations for 70,003 abortions adds up to only a 1.3% rate of hospitalization due to complications. Given how often abortion opponents emphasize the dangers of abortion, this number actually seems really low.
Some my find it surprising that 6% of those who have first trimester medication abortions have complications requiring hospitalization. However, this number is more complicated than it appears. While the 6% figure is used in that line, the number of women hospitalized listed is only 3%. As the note at the bottom explains, this is because the 6% statistic actually refers to the percentage of those who had to follow their medication abortion with a surgical abortion because the medication abortion did not complete, not to the percentage of women hospitalized. The number of women hospitalized is based on the assumption that half of those whose medication abortions do not complete will have their surgical abortion followup at a local hospital rather than at an abortion clinic.
Individuals who choose medication abortions are told up front that there is a small chance that the pills (which they take at home) will not be fully effective, and that in that case they will need to come in and follow the procedure up with a surgical abortion. The followup is routine, and is typically the result of the failure of the pills to complete the abortion, not life-threatening bleeding or other complications. In other words, while some percentages of these followup surgical abortions may occur in a hospital, they are simply a repeat abortion procedure and not blood transfusions or life support.
When we understand that the majority of the 6% figure for complications requiring hospitalization listed under first trimester medication abortions refers to those who have to follow their medication abortion with a routine surgical abortion, the risk listed for first trimester abortions declines quite a bit. Even with this understanding, however, medication abortions are still associated with more risk than surgical abortions. A proper response to this reality should be to (a) fund research to make the abortion pill safer and (b) promote the safer surgical abortions and make these surgical abortions more widely available, which are both things abortion opponents oppose.
It is well known that second trimester abortions have a greater risk of complications than first trimester abortions. Because of this, I don’t find the 6% rate of complications requiring hospitalization all that surprising. Because second trimester abortions are more risky, I support making first trimester abortions more readily available. A significant number of individuals who have second trimester abortions do so because they were unable to access an abortion during their first trimester, often due to accessibility or financial need. If we make first trimester abortions more accessible, we can substantially cut down on the number of second trimester abortions and thus cut down on the health risks involve—but this is exactly what abortion opponents are fighting to stop.
Even with the slightly higher rate of complications for medication abortions and the significantly higher rate of complications for second trimester abortion, the overall rate of hospitalization from complications due to abortion in Texas is only 1.3%. This number is far lower than the typical rate of hospitalization after an outpatient surgery center, yet Republicans are working to expand the number of outpatient surgery centers. If Republicans see outpatient surgery centers as a safe, cost-effective alternative to surgeries performed in hospitals, in spite of these centers’ substantially higher rate of hospitalization due to later complications, why all the fuss about abortion clinics, which follow essentially the same model and are in fact safer than outpatient surgery centers?
There’s something else that suggests that it’s not really about protecting women’s health as well. While roughly 1.3% of those who have abortions are hospitalized due to complications, nearly 100% of those who carry their pregnancies to term are hospitalized. In other words, if those 70,003 individuals had not had abortions, they would for all intents and purposes all have been hospitalized. Now yes, many would argue that childbirth is a natural process and should not be seen as a “complication.” Still, the rate of complications from pregnancy is not negligible, and in 2011 there were 30.7 maternal deaths per 100,000 live births. If abortion had the same mortality rate, we would have seen 21.5 deaths due to abortion in Texas in 2011, when instead there were zero.
Abortion is far safer than birth. Troy Newman of Operation Rescue calls 1000 hospitalizations due to abortion in Texas each year “completely unacceptable.” What does he think of the 116 women who died in childbirth in Texas in that same year? While researchers are still discussing the reasons for the U.S.’s unusually high maternal mortality rate, most agree that lack of access to healthcare is a significant part of the problem. And yet, Republicans have blocked both medicaid expansion and other proposals that would extend healthcare to pregnant individuals. If abortion opponents truly cared about women’s health, they ought to support policies that would make pregnancy and maternity care more affordable and more available—and they need to acknowledge that pregnancy and childbirth are far more risky than abortion, and act like they actually believe that.
Let’s finish by talking for a moment about the controversy over admitting privileges. A Texas law passed in 2013 required abortion doctors to have admitting privileges at a local hospital at any clinic where they provide abortions. On some level, this law sounds well meaning and reasonable. However, because of a decades-long campaign of terror against abortion doctors, many clinics are unable to find a local doctor willing to perform abortions. Further, the shortage of doctors willing to perform abortions and the stigma against abortion doctors means that doctors who do proally gvide abortions often end up only providing abortions. Many abortion doctors travel from clinic to clinic providing abortion services for individuals who wound not otherwise have access to an abortion provider. Requiring these doctors to have admitting privileges at numerous hospitals across the state is neither practical nor necessary, especially given the overwhelmingly safe nature of the procedure.
Abortion opponents would have you think that abortion doctors practicing at abortion clinics without having admitting privileges at a local hospital is profoundly medically dangerous, but this misunderstands the current situation. In my own town, our local Planned Parenthood offers abortions only one day a week. That day, an abortion doctor travels to my town from a nearby city. The Planned Parenthood clinic has an arrangement with a local doctor who would take over the care for any patient who has to be transferred to the hospital in case of an emergency. I am not sure whether this is common practice more generally, but hospital emergency rooms are required to accept and treat all patients regardless of whether the doctor who originally treated them has admitting privileges.
And if this isn’t enough to convince you, the American College of Obstetricians and Gynecologists (ACOG) and the American Medical Association (AMA) filed a joint amicus brief in support of Planned Parenthood’s challenge to the Texas admitting privileges law. Troy Newman of the anti-abortion group Operation Rescue has written that “[r]equiring local hospital privileges is a way to protect women and save lives until such time as the practice of abortion can be completely abolished,” making the true intent of such laws clear. The “lives” Newman writes of saving are the lives of the fetuses who will no longer be aborted, because the true intent of admitting privileges laws is to shut down abortion clinics, not to protect women’s health.
Note: I have used the term “women” as it refers to the terms used in the graph and have spoken of “women’s health” in the context of anti-abortion framing of this discussion. In all other cases I have sought to use gender neutral language to reflect the reality that anyone with functional ovaries and a uterus can become pregnant.